
Occipitocervical Fusion Surgery
Advanced Stabilization for Complex Upper Cervical Spine Disorders
Understanding the Craniovertebral Junction (CVJ)
The craniovertebral junction is where the base of the skull meets the first two cervical vertebrae (atlas and axis). This region:
Supports the head
Enables head rotation and nodding
Protects the brainstem and upper spinal cord
Maintains neurological function
Even minor instability in this area can cause serious neurological symptoms because vital structures such as the brainstem, spinal cord, and vertebral arteries pass through this region.
When instability occurs and conservative treatment fails, occipitocervical fusion becomes necessary.
What Is Occipitocervical Fusion?
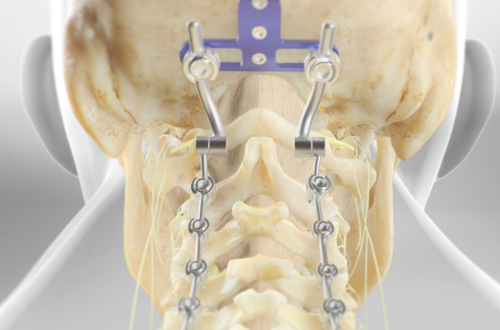
Occipitocervical fusion is a surgical procedure that permanently stabilizes the connection between the skull and upper cervical vertebrae using:
Titanium screws
Rod systems
Plates
Bone graft material
The goal is to eliminate abnormal motion, relieve pressure on the spinal cord, and restore structural alignment.
This surgery is considered when instability threatens neurological function or causes severe pain and disability.
Conditions Treated with Occipitocervical Fusion
Dr. Alok Gadkari performs occipitocervical fusion for a range of complex spinal conditions, including:
1. Traumatic Injuries
Fractures of C1 or C2
Ligament rupture
Dislocations at the craniovertebral junction
Severe trauma from accidents can cause instability requiring urgent surgical stabilization.
2. Rheumatoid Arthritis
Advanced rheumatoid arthritis can damage ligaments and bones of the upper cervical spine, leading to atlantoaxial instability.
3. Congenital Abnormalities
Basilar invagination
Atlantoaxial instability
Os odontoideum
Klippel-Feil syndrome
These conditions may compress the brainstem or spinal cord.
4. Tumors
Primary or metastatic tumors affecting C1–C2 or the skull base may require fusion after tumor removal.
5. Degenerative Conditions
Severe cervical spondylosis or instability unresponsive to conservative treatment.
6. Infection
Infections such as tuberculosis or osteomyelitis that destroy bone stability.
Symptoms That May Indicate Need for Surgery
Patients with craniovertebral instability may experience:
Severe neck pain
Occipital headaches
Difficulty walking
Hand weakness or numbness
Loss of balance
Difficulty swallowing
Tingling in arms
Signs of spinal cord compression
Progressive neurological deficits
If untreated, compression at this level can lead to serious neurological impairment.
Early diagnosis and surgical intervention can prevent permanent damage.
Diagnostic Evaluation
Dr. Alok Gadkari performs detailed evaluation before recommending surgery, including:
Clinical Examination
Neurological assessment
Muscle strength testing
Reflex evaluation
Gait analysis
Imaging Studies
X-ray (dynamic flexion-extension views)
MRI scan
CT scan
3D reconstruction imaging
CT angiography if needed
Precise imaging is critical because this region is anatomically complex and houses vital structures.
Surgical Procedure: Step-by-Step Overview
Occipitocervical fusion is performed under general anesthesia.
Step 1: Positioning
The patient is placed carefully to maintain spinal alignment.
Step 2: Posterior Approach
A small incision is made at the back of the head and upper neck.
Step 3: Exposure
The surgeon carefully exposes the occiput and upper cervical vertebrae.
Step 4: Instrumentation
Screws are inserted into the occipital bone
Screws are placed into C1, C2, or lower cervical vertebrae as required
Rods connect the screws to create rigid fixation
Step 5: Bone Grafting
Bone graft (autograft or synthetic) is placed to promote fusion between the bones.
Step 6: Closure
The incision is closed in layers.
The surgery typically lasts 2–4 hours depending on complexity.
Goals of Occipitocervical Fusion
Stabilize unstable vertebrae
Relieve spinal cord compression
Prevent neurological deterioration
Correct deformity
Reduce severe pain
Improve quality of life
The fusion eliminates movement at the affected levels, which protects the spinal cord and brainstem.
Benefits of Surgery with Dr. Alok Gadkari
Advanced spinal instrumentation
Precision-based surgical planning
Comprehensive neurological monitoring
Evidence-based surgical protocols
Patient-centered approach
Detailed post-operative rehabilitation planning
With specialized expertise in complex spine procedures, Dr. Gadkari ensures maximum safety and long-term stability.
Recovery After Occipitocervical Fusion
Hospital Stay
Patients typically stay in the hospital for 3–7 days.
Immediate Postoperative Phase
Neck brace may be advised
Pain management protocols
Early mobilization with support
First 6 Weeks
Gradual increase in activity
Avoid heavy lifting
Wound care monitoring
3 Months
Fusion process continues
Improved neurological symptoms
Physical therapy begins
6–12 Months
Solid bone fusion forms
Most patients return to regular daily activities
Full fusion may take several months to complete.
Life After Occipitocervical Fusion
Most patients experience:
Significant pain relief
Improved balance
Better neurological function
Increased confidence in daily activities
Certain movements such as extreme neck rotation will be limited permanently due to fusion.
However, patients adapt well and report improved quality of life.
Why Early Treatment Is Important
Delay in treating craniovertebral instability can result in:
Progressive spinal cord damage
Irreversible neurological deficits
Difficulty walking
Breathing problems in severe cases
Timely surgical stabilization prevents long-term disability.