
Posterior Cervical Spine Surgery
Advanced Neck Spine Treatment by Dr. Alok Gadkari
Understanding the Cervical Spine
The cervical spine consists of seven vertebrae (C1–C7) in the neck region. It supports the head, allows movement, and protects the spinal cord and nerve roots.
When structures in this region compress the spinal cord or nerves, patients may experience:
Persistent neck pain
Radiating arm pain (cervical radiculopathy)
Numbness or tingling in hands
Muscle weakness
Difficulty in coordination or walking
Balance issues
Loss of fine motor skills
Posterior cervical spine surgery is performed from the back (posterior) side of the neck to relieve pressure on the spinal cord or nerves and stabilize the spine when needed.
What is Posterior Cervical Spine Surgery?
Posterior cervical spine surgery is a surgical approach performed through an incision at the back of the neck. It allows the surgeon to:
Decompress the spinal cord
Remove bone spurs or thickened ligaments
Treat cervical stenosis
Remove tumors or infections
Stabilize unstable spinal segments
Correct certain deformities
Dr. Alok Gadkari carefully evaluates each patient to determine whether the posterior approach is the most suitable surgical option.
Conditions Treated with Posterior Cervical Spine Surgery
Dr. Alok Gadkari performs posterior cervical procedures for various spinal disorders, including:
1. Cervical Spinal Stenosis
Narrowing of the spinal canal causing pressure on the spinal cord.
2. Cervical Myelopathy
Compression of the spinal cord leading to weakness, imbalance, and coordination problems.
3. Cervical Radiculopathy
Nerve root compression causing arm pain, tingling, or weakness.
4. Ossification of Posterior Longitudinal Ligament (OPLL)
Abnormal thickening of ligament causing spinal cord compression.
5. Cervical Disc Prolapse (Selected Cases)
Certain disc herniations requiring posterior decompression.
6. Cervical Fractures or Instability
Trauma-related instability requiring stabilization.
7. Tumors or Infections
Spinal lesions requiring decompression and removal.
Types of Posterior Cervical Spine Surgery
Depending on the diagnosis and severity, Dr. Alok Gadkari may recommend one of the following procedures:
1. Cervical Laminectomy
This procedure involves removing the lamina (back part of vertebra) to create more space for the spinal cord.
Benefits:
Effective for multilevel spinal cord compression
Relieves pressure in cervical stenosis
Improves walking and coordination
Sometimes laminectomy is combined with spinal fusion for stability.
2. Cervical Laminoplasty
Instead of removing the lamina, the surgeon reconstructs and expands it to enlarge the spinal canal.
Advantages:
Preserves spinal stability
Maintains some natural movement
Suitable for multilevel stenosis
Dr. Alok Gadkari selects laminoplasty for appropriate patients to maintain mobility.
3. Posterior Cervical Foraminotomy
This minimally invasive procedure removes bone or soft tissue compressing a nerve root.
Ideal for:
Cervical radiculopathy
Arm pain due to nerve compression
Single-level pathology
It often preserves spinal motion and avoids fusion.
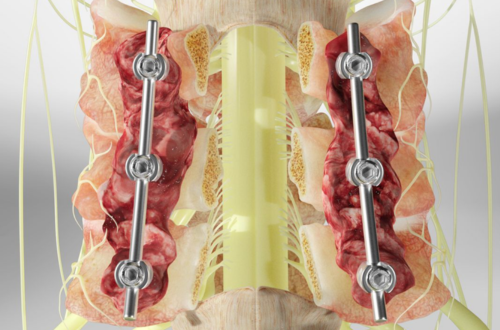
4. Posterior Cervical Fusion
Fusion stabilizes unstable spinal segments using screws and rods.
Recommended for:
Spinal instability
Severe degeneration
Fractures
Post-laminectomy instability
Fusion provides long-term stability and prevents abnormal movement.
Symptoms That May Require Surgery
Seek evaluation if you experience:
Persistent neck pain for months
Arm pain not responding to treatment
Progressive weakness
Difficulty walking
Loss of balance
Hand clumsiness
Bladder or bowel changes (urgent condition)
Early surgical intervention can prevent permanent neurological damage.
Pre-Surgical Evaluation by Dr. Alok Gadkari
Before surgery, patients undergo:
Detailed neurological examination
MRI scan of cervical spine
CT scan (if required)
X-rays with flexion-extension views
Blood tests
Pre-anesthesia fitness evaluation
Dr. Alok Gadkari explains all surgical options and tailors the treatment plan individually.
The Surgical Procedure – What to Expectery
Step 1: Anesthesia
General anesthesia is administered.
Step 2: Positioning
Patient is positioned face down carefully to protect nerves and airway.
Step 3: Incision
A midline incision is made at the back of the neck.
Step 4: Decompression
Bone, ligament, or disc material compressing the spinal cord is removed.
Step 5: Stabilization (if required)
Screws and rods may be placed for fusion.
Step 6: Closure
The incision is closed carefully with sutures.
Surgery duration depends on number of levels involved.
Benefits of Posterior Cervical Spine Surgery
Patients treated by Dr. Alok Gadkari experience:
Relief from arm pain
Improvement in walking ability
Better hand coordination
Reduced numbness
Improved balance
Prevention of neurological worsening
Improved quality of life
Timely surgery can halt progression of cervical myelopathy.
Recovery After Posterior Cervical Spine Surgery
Immediate Post-Operative Period
Monitoring in recovery room
Pain managed with medications
Early mobilization encouraged
Hospital Stay
Typically 3–5 days depending on complexity.
Neck Support
A cervical collar may be advised temporarily.
Physiotherapy
Gentle exercises
Strengthening program
Posture correction
Return to Work
Desk jobs: 3–6 weeks
Physically demanding jobs: 8–12 weeks
Recovery varies based on condition and number of levels treated.
Posterior Cervical Surgery vs Anterior Cervical Surgery
| Feature | Posterior Surgery | Anterior Surgery |
|---|---|---|
| Approach | Back of neck | Front of neck |
| Best For | Multilevel stenosis | Single-level disc |
| Motion Preservation | Possible in laminoplasty | Limited |
| Fusion Required | Sometimes | Often |
| Recovery | Slightly longer | Usually faster |
Long-Term Outcomes
Studies show that posterior cervical decompression significantly improves:
Neurological function
Walking ability
Arm strength
Quality of life
Early surgery gives better results in cervical myelopathy cases.
Patients are followed regularly to monitor recovery and spinal stability.